
Understanding pandemic-emergent personality & behavioral psychopathology.
Social media amplification

There is not a more direct and clear way to introduce the topic of this post than by sharing the following tweet which is profound in its simplicity:
The latest round of acute COVID hysteria over a new mutant variant of the SARS-CoV-2 virus (#B11529) was the final nudge I needed to write this post to hopefully help provide insight into the diverse human behavioral and psychological reaction to the pandemic and what such reactions may reveal about individual differences in sensitivity to environmental context. As my scientific work is largely in the field referred to as developmental psychopathology, I draw on concepts and theories that have generated much thinking and research within it. Broadly speaking, developmental psychopathology is an academic field of research and scholarship that examines the development of mental illness symptoms and disorders across the life course and the biological, social, and cultural factors that may give rise to and maintain them.
Although my initial thinking on the behavioral response to the pandemic centered around a differential susceptibility1 to environmental influences model as possessing significant heuristic and explanatory value, I am now strongly inclined to think the classic diathesis-stress model possesses the most explanatory value (and is the more efficient or parsimonious of the two models) for the marked emergence of anxiety and fear in a distinct class of the population. Although beyond the scope of this piece, it should be noted that these models, as well as other models of the development of psychopathology (e.g., the stress inoculation model), overlap both in terms of the thinking behind them as well as the predictions they make, and thus adoption of one model to explain population-level human phenomena should not be seen as necessarily excluding the others.
Below I discuss the diathesis-stress or dual-risk model of sensitivity to environmental context, how it relates to the pandemic and individual behavioral responses to it, and offer some broader, loosely organized observations with especial reference to a more general conceptual notion of sensory processing sensitivity and “Long COVID”.
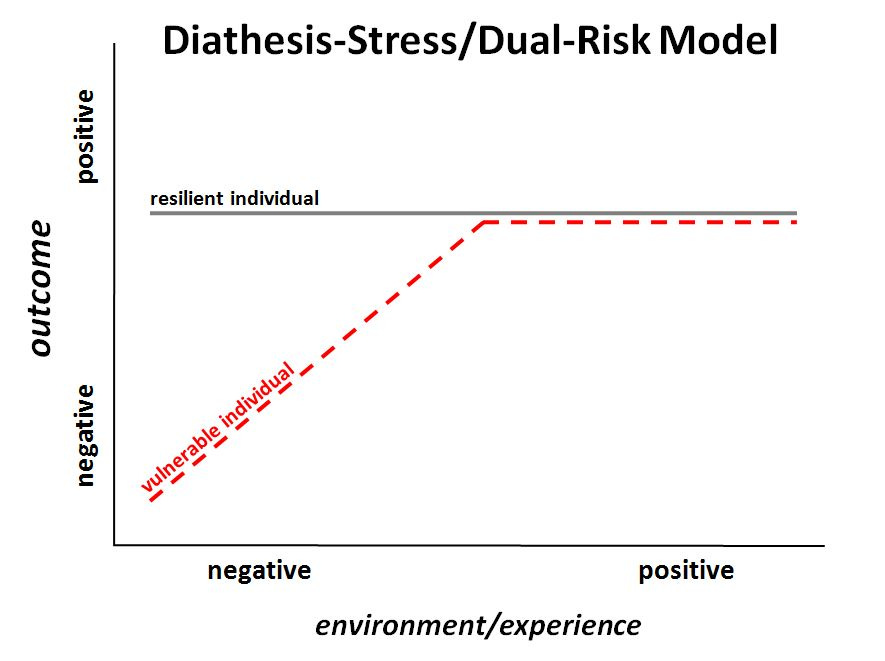
Within developmental psychopathology, the classic diathesis-stress or dual-risk model postulates that poor developmental experiences (e.g., abusive parenting or resource poor stressful environments) more strongly impact the development of individuals who carry vulnerability factors, which are ‘latent’ (unobserved) diatheses that increase risk for psychopathology when “triggered” by exposure to negative developmental experiences or—more broadly—stressful environments. Latent diatheses reflect biological or social-cognitive predispositions to react and behave in specific ways; psychopathology reflects symptoms and behaviors associated with mental illness, such as high levels of anxiety, panic, and so forth.
A given individual may possess a higher or lower sensory threshold for experiencing anxiety and panic in the context of a single stressor or stressful experience—or a broader, sustained stressful environment such as that associated with the pandemic—dependent upon biologically-based reaction thresholds that are thought to be largely genetically determined. From this, it is straightforward, then, to see that those with a lowered threshold for experiencing the constellation of clinical and personality symptoms and behaviors associated with emotional lability and affective dysphoria would be more vulnerable in the context of the COVID-19 pandemic.
It has now been over a year and a half since the emergence of COVID-19 and the virtually non-stop media coverage of the pandemic and its sequelae (lockdowns, NPIs, vaccine development, vaccine mandates etc.). It has become quite clear, both in real life (just take a trip to your local supermarket, for example) and especially in the social-media metaverse—that a distinguishable segment of the population has reacted and continues to react to the ongoing pandemic with a heightened sense of anxiety, panic, fear, neuroticism, and often authoritarian calls for societal responses that are excessively restrictive and either explicitly or implicitly predicated on a notion of “Zero-Covid.” Moreover, in addition to messages and decision-making from institutional authorities, social media, especially Twitter, has served as conduit, amplifying the emotive resonance of such affective tonicity into a collective hysteria by glossing it with a semblance of what is arguably a performative theatric narcissism (especially as it relates to masking) intended to generate social media attention and traffic while simultaneously casting opprobrium on those who do not share the same degree of alarmism.

In the words of American sociologist and cultural critic Philip Rieff, who seemingly presaged this cultural phenomenon:

Mental illness symptom and trait dimensions vs. categorical disorders.
To fully appreciate the pandemic-induced emergence of a collective anxiety and neuroticism, it is crucial to understand that, unlike most medical conditions with a clear demarcation between the disease and non-disease state (i.e., an identifiable physical basis), most psychological ‘disorders’ (i.e., as defined in the DSM or the ICD) are not natural kinds, but rather have been treated as such given they are useful heuristics for clinical practice and research. That is, they have been reified as natural kinds to accommodate grant-making bodies, journal reviewers and editors, and to guide treatment and eligibility for insurance reimbursement. Instead, genetically-informed studies have provided evidence that the genetic variants associated with most psychological symptoms and conditions are distributed normally in the population.
The clinical phenotypes (symptom presentations) of most psychological disorders also appear to be distributed normally in the population (rather than categorically); broadly speaking, each one of us has a greater or lesser tendency to experience anxiety, sadness, neuroticism, and so on—our thresholds for experiencing these psychological symptoms and traits exist ‘on a spectrum’. Another way of stating this it is that it is normal to feel sad, anxious, mad, happy, etc. at anytime. Some of us may even have a few extra thoughts of worry/anxiety or sadness/depression. These normal experiences become pathologic when they occur with such frequency and intensity that they interfere with one’s life and the ability to enjoy their life.
The above discursion is important because it provides a conceptual platform from which one is hopefully better able to understand why individual elevations in these symptom traits will be observable irrespective of a psychological disorder diagnosis per se. When examined at the level of the population (i.e., in aggregate), observable behavioral phenomenon in distinct population subclasses become more apparent. Perhaps the most readily identifiable such ‘subpopulation’ is that of biological sex which has clear associations with pandemic behavioral response given the reliable association between biological sex and distinct patterns of phenotypic expression of several psychological symptoms and traits, perhaps most especially internalizing symptomatology (anxiety, depression, etc.).
The Case of Long COVID.
Long COVID (also called long haulers and post-acute COVID syndrome) is a quasi-medical term that refers to persisting symptoms following COVID-19 that include, intermittent headaches or tiredness, as well as other common clinical symptoms associated with various mental illnesses. Indeed,
In addition to a loosely operationalized syndrome of a wide-range of behavioral, psychological, and somatic symptoms, virtually all of the empirical work to date on long-COVID is plagued by methodological limitations and shortcomings, most notably the lack of adequate control groups and a lack of adjustment for pre-existing psychiatric symptomatology (pre-COVID case designation) in the individual. These shortcomings are crucial to correct and overcome if a firm understanding of the empiric reality of a long-COVID syndrome that is causally related to a rigorous gold-standard operationalization of COVID-19 diagnosis (e.g., RT-PCR). What may be more plausible in light of the above discussion of the diathesis-stress model is that current ‘Long-COVID’ is rather the amplification of a pre-existing diathesis for a propensity to experience emotional lability and symptoms of affective dysregulation (e.g., anxiety, panic, fear) that is masquerading as unique and ‘novel’ condition associated with the SARS-CoV-2 virus itself. It is worth nothing that one systematic review has identified biological sex as a likely risk factor for long COVID which, as noted above, also is associated with symptoms of clinical symptomatology that are at the heart of the intense emotional and behavioral response to the pandemic observable in a subclass of the population.
What is a reasonable societal level of vigilance? NPIs, VAXX mandates, & proportional risk.
As one Twitter acquaintance of mine noted in conversation with me on the issue of NPI intervention strategies to the ongoing pandemic:
“severe NPIs for a respiratory illness who’s spread cannot be realistically controlled [at the level of the population] and a <0.1% aggregate fatality rate in those under 70yo require devolution into gaslighting and a fear campaign.”
NPIs were considered as universal mandated masking, lock downs, and related features (school closures, travel restrictions). Mandating universal masking, especially in young children and adolescents for whom the virus poses minimal risk either to the self or as a vector of transmission (less efficient transmitters) to higher-risk groups, is especially concerning given the potential impacts on social communication and emotional development. This is especially the case for children with learning disabilities and other developmental concerns. (e.g., visualizing phonation of words).
Mandated vaccinations, including vaccine passports, and endless iterations of what is considered ‘fully vaccinated’ likewise raise the specter of societal responses that are disproportionate to the true level of risk posed by the virus.
All of the above exaggerated responses are magnified when one considers the social and behavioral consequences of both over-aggressive NPI response policies in the population and mandated vaccination policy, especially for particular subpopulations (e.g., young adolescent males). The irrationality of such policies are further amplified by a denial by public health authorities as to the effectiveness of natural immunity to the virus. A functional society can not be mired in fear if it expects to end the pandemic which equates to learning to live with an endemic virus. Sensible off-ramps that emphasize fewer restrictions guided by a pre-pandemic way of life are needed. However, to the degree that a society’s ruling class is comprised of and influenced by a polity (which presumably placed them in a position of power) that are disproportionately more likely to carry a latent vulnerability to experience anxiety, fear, and a more general lowered threshold for emotional lability, the more likely a panic-laden, punitive, and ultimately inefficient response to the pandemic is likely to result.
Diathesis-stress processes are almost certainly a likely driver of pandemic behavioral response among a subset of the population, which in turn disproportionately influences media coverage and policy decisions. Armed with this insight, what is a balanced, sensible, and reasonable societal risk analysis and response to the pandemic at this point in time given the availability of vaccines, reasonable vaccination rates, and the recognition that Zero-Covid was never even remotely a realistic possibility and that the virus will become endemic?
The answer is a response that focuses on the population—the vast majority of whom will face minimal risk from the virus—and that minimizes unintended harms associated with unfocused or ineffective control efforts. Encouraging vaccination uptake in the elderly and other high-risk groups (optimizing vaccine rollout), encouraging outdoor activities, and reinforcing (though not over-emphasizing) basic hygiene and social practices that were commonsense pre-pandemic to limit virus and pathogen spread (e.g., washing hands, covering your mouth when sneezing, and remaining home when sick) should be highlighted.
What is not balanced, nor healthy, is a hysteria-driven, fear-based media ecosystem that drives a faux existential crisis. Such an ecosystem further polarizes the polity based on pre-existing latent vulnerabilities to emotional lability—the clinical symptoms and personality traits of which themselves show associations with both political ideology and political party affiliation—and increasingly frustrates the majority of the population.


Accurate and proportional risk assessment of the virus and a wholesale understanding that returning to a sensible pre-pandemic normalcy will likely improve quality of life and mental functioning for most of the population is needed. A continually high COVID panic meter is untenable. Bringing us full circle, the following tweet from Dr. Kaur is similarly profound in its simplicity:
I am a special eduction teacher and in the spring of 2020 as I sat at home watching my students struggle learning via computer I developed a hypothesis that I have seen come to fruition. I told my husband that people we know and people we don’t know and might have gone the rest of our lives interacting with in normal circumstances had begun to exhibit a level of fear and paranoia that was shocking. My theory was that this instability (for lack of a better word) had always been there and we might never have seen it, but for the trigger of Covid. It was now oozing from their pores, making them completely unstable and hysterical. A dear friend mentioned in casual conversation he had been tested 25+ times (that’s just nuts). We were saddened but not really surprised because his neurosis had been evident for a while. My husband said “that’s pure fear and hysteria.” That’s what has been so difficult, to watch people we love and care about descend into a kind of madness that we are helpless to bring them out of, because they refuse any logic and reason. Thank you for this essay. It is comforting to know I wasn’t alone all this time.
I've found in my clinical practice that the less emotionally resilient patients who have succumbed to this pandemic of fear largely share one additional trait--lack of curiosity. They ask no questions and have no interest in pursuing answers. Curiosity inoculates against this type of hysteria.